If you have been to the page, you may have noticed I have recently changed the avatar from dr zoidberg. The new one is pretty neat and zoidberg could use some time off. It looks almost like me…an almost, ALMOST dr j ![]() To give credit where credit is due, thanks be to carmen, who pointed me to maebemaebenot who actually found this hot new trend all the kids these days are doing. And in case you also want to jump off this bridge all the popular kids are leaping from, here is the link for yourself
To give credit where credit is due, thanks be to carmen, who pointed me to maebemaebenot who actually found this hot new trend all the kids these days are doing. And in case you also want to jump off this bridge all the popular kids are leaping from, here is the link for yourself
Other than that, the rotation is going as well as can be expected. Managed to see a case of eye herpes on a 67 year old woman. You are wondering how she got it, perhaps? disturbed by the thought of a granny getting freaky? Well, set your minds at ease, because she had type 1, the oral variety. She had touched her lip during a recurrence, and then touched her eye without thinking about it.
Now that happens to be a far more severe case than what I saw. But do you notice the growth of blood vessels and advancement of the sclera (white part of the eye) onto the cornea? That is known as neovascularization. It is one of the common signs of a herpetic infection in the eye.
The lesson: Wash your hands. Also, dont get herpes, if you can help it.
I also got to see a couple of cataract lens removal patients, preoperatively all the way through to post op. In cataracts, the lens of your eye accquires opacities as you age, kind of like a window pane building up dirt over the years. Now some people it affects so severely that they can no longer see through the window. So that is when we go in, remove the old lens, and put in a new one. Like smashing the window open, taking out all the glass, and putting in a new window. But since I am using a retrospectively poor simile,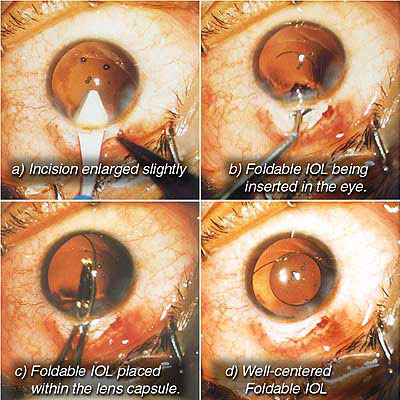
And without using a slit lamp to examine a dilated eye, you would never know the difference. Creepy, isn’t it?
Most of the remaining patients were rather routine…yearly vision exams, follow up diabetic and/or glaucoma appointments, an occasional red eye or contact lens fitting, nothing to write home (or the internet) about. I use these patients to learn more about common problem management, and improve my ability with direct fundoscopy…using the handheld I am now almost always able to find the optic disc and nerve, and am gradually improving in my ability to estimate cup/disc ratio, and some indirect fundoscopy, which is the same as direct, only not. ![]()
Have you ever been in a car and heard or used the phrase “pedestrian! 10 points!” or some equivalent thereof, and wondered where it comes from? Wonder no more…the concept of numerary reward for hit and runs dates back to a 1975 film titled “Death Race 2000″. Costarring a young sylvester stallone. In a postapocalyptic world, the united provences entertain the masses with a cross country death race. Racers are awarded points not only for winning, but also for number of pedestrians destroyed with the elderly and the pediatric given higher values and such. 

Incidentally, a remake of that film will be released next friday simply entitled “death race” I am interested to see how the story is adapted. I advise you to watch the original and compare for yourself.
As for the weekend, I have been on a five mile hike at silver falls state park, which i will go into more detail about next post. I will also be heading up to Portland to check out the zoo, the remainder of the city and go to the indian festival being held that day…I dont know how i keep coming across these random ethnic festivals, but i am not complaining ![]()
in answer to the olympics post, the fake story was the one about lack of compelling human drama disqualifying an athlete. Below is another article from the same writer, andy borowitz
China’s Gold Medals Found to Have High Lead Content
China’s impressive haul of gold medals at the Beijing Olympics was
tarnished somewhat today when it was revealed that “abnormally high
levels of lead” were found in the first-place medallions.
The medals, which were supposed to be made entirely of gold, were
instead found to be composed of 99% lead alloy and coated with a
gold-colored lead-based paint.
The shocking revelations roiled the Olympic complex today and sent
officials looking for answers from the Chinese manufacturer of the
medals, the Wuhan One Hundred Percent Gold Medal Corporation.
“We are trying to determine how exactly so much lead got into those
gold medals,” said a spokesman for Wuhan, China’s largest exporter of
gold medals. “Until we do, we are urging all first-place athletes not
to lick, taste or suck on their medals.”
The news about the potentially toxic gold medals spread panic among
Olympic champions, especially U.S. swimming phenom Michael Phelps.
“I am very, very concerned about my extensive contact with gold
medals,” Mr. Phelps told reporters. “But what am I supposed to do? Stop
being so awesome?”
In other Olympic news, China’s hopes for winning more medals in
women’s gymnastics were dashed when one of their leading gymnasts
vanished down a bathtub drain on Tuesday.
Immediately after Jiang Qimin’s disappearance, Beijing authorities launched a search for the acclaimed seven-pound athlete.
Jiang had been the subject of speculation earlier this week as many
foreign observers doubted China’s claims that the two-foot-tall gymnast
was sixteen years old.
In an interview with NBC’s Bob Costas on Monday, Jiang sparked
controversy with this response to a question about her age: “I want my
sippy cup.





































Recent Comments